These data are obtained from the Brazil Ministry of Health microcephaly reports, which you can also find here.
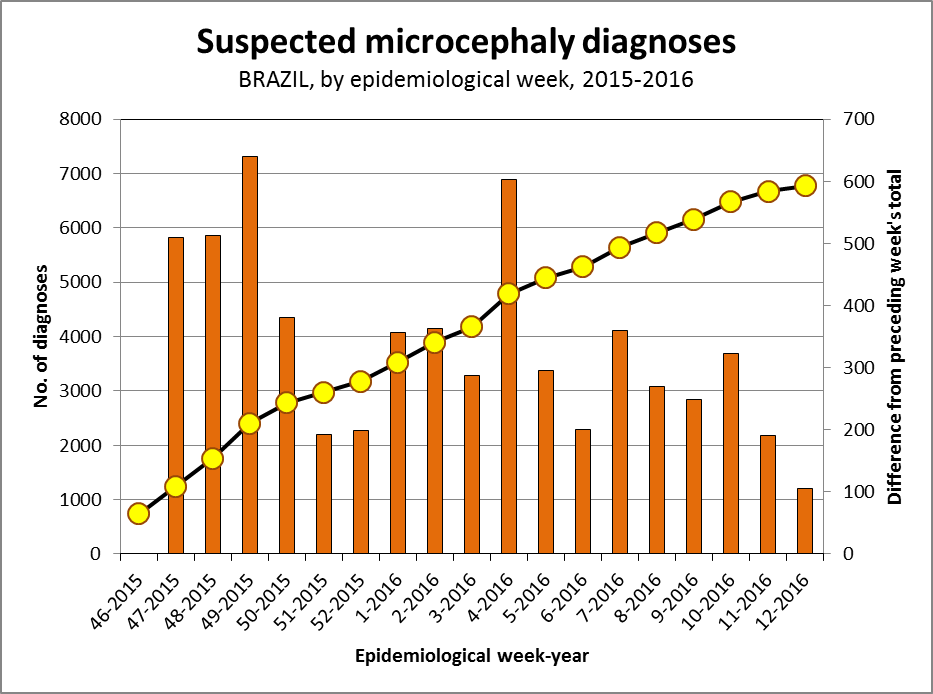
Above we can see a cumulative curve (black line, yellow dots read using the left-hand axis) which adds each week's cases to the total from the week before. The curve appears to be rounding off in in the last few weeks which might suggest a slowing of the rise in number of microcephaly diagnoses.
Or it might be too early to say.
The vertical orange bars (read against the right-hand axis) are the differences between reports. The first bar is the total diagnoses in week 54 of 2015, minus the total from week 46, 2015, and so on. There seem to be fewer new cases each week over the last 3 epidemiological reporting weeks.

We see the rise in discarded suspected microcephaly diagnoses (blue; they were classified as not being microcephaly cases) which became a little steeper between Week 7-10.
Confirmed microcephaly diagnoses (red) did not rise as steeply and seem to have slowed in the last 2 reporting weeks.
The number of laboratory confirmed Zika virus positives (green) among the confirmed microcephaly diagnoses is much smaller and oscillates.
This chart also shows that these extra details didn't start appearing until around Week #2 of 2016.




















